")
")
")
")
")
")
")
")
")

Bioenergetic Analysis in Psychosomatic Medicine. Short-Term Bioenergetic Therapy
Author: Thomas Ehrensberger | Published in: IIBA Clinical Journal - Issue: 1987 - Volume 2 - Num 2 | Date of publication: 1987
Click here to read the article in PDF format ...
![]()
1. INTRODUCTION
Bioenergetic Analysis is a psychosomatic approach to the patient. Psychosomatics is a relatively new term for an access to medicine and describes a way of looking at the patient which is probably as old as the healing arts themselves: "It is not a speciality, a special medical branch, but a way of looking which covers all branches of medicine, even surgery. Psychosomatics does not mean that we are giving less attention to somatic aspects, but that we are giving more attention to the psychic part of the person. Psychosomatics puts the emphasis on the old principle of unity of body and soul, of interdependence of both, a view which always was leading the wise physician."
(This definition comes out of the first book on psychosomatic medicine, published in 1943 in England by the internist WEISS and the psychiatrist ENGLISH). It was the medical profession that was looking for a way to integrate psychological fact sand research to the more somatic approach in medicine. For many purely somatically oriented physicians the term psychosomatics means that wellknown pathways of scientifically based facts will be left, and many of our colleagues believe that psychosomatics are dealing with magic or esoteric phenomena.
2. THEORETICAL CONCEPTS IN PSYCHOSOMATIC MEDICINE
Many different theoretical concepts have been presented and as an example I would like to describe the "circle of situation" ("Situationskreis") described by Thure von UEXKULL, a father of psychosomatic medicine (1).
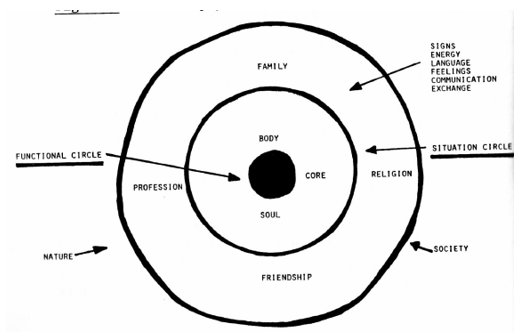
Figure 1: Somato-psycho-social-reality
In this theoretical concept the specif Ir difficulty of the therapist working with a psycho
somatic approach is described. The term "circle situation" means that the reality of each Individual, his expressive movements, and the echoes of his messages are a subjective world, which in no way can be reconstructed, repeated or adapted from one individual to another. The person exists not only as a body-soul organism, but is embedded in his personal life where he always is in contact with messages and echoes with his surroundings. The "functional circle" ("Funktionskreis") means the dimensions of the more animal functions. The biological nature, the facts of doing something and creating reactions, the instincts and the inherited Information. Orthodox medicine deals with the functional circle, psychosomatic approach with the cIrcle of situation, the individual reality or the picture of reality designed subjectively by every patient. What we have as information about a patient are signs and symbols for his own and unique way of dealing with his world. So every person creates his own reality. Doing therapy means reading signs and i lien responding with our signs and symbols, which again come out of our own unique perception of the world. Von UEXKULL has called this phenomenon the "arena" of the human being, so when we meet a patient, our own arena meets the arena of another person and we exchange signs, which hopefully will help both to clarify their world and to find a way nut of traps and constrictions. This is a mutual demand of each patient, when he comes to see a therapist.
In bioenergetics, we learn to look for blocks, that means to look for areas in the body where energy is influenced in a painful way. Psychoanalysis looks for conflicts and only in a therapy in which conflicts or blocks are worked on, will we really help the patient. The being there, the nurturing, must be well-balanced with a more painful work with resistances.
3. WORKING WITH UNMOTIVATED PATIENTS
I think that the wide range of bioenergetic therapists work very little with real psychosomatic patients. We are used to working with psychosomatic symptoms but, believe me, very few psychosomatic patients will ever seek help from a psychotherapist. Most of the bioenergetic therapists I know are psychiatrists or psychologists, which means they are specialists for the psychic (in the view of the patient).
Between 50 and 70 percent of patients in a general practice or a practice of internal medicine are psychosomatic. About one-third of them are constantly on the trip from one physician to another, looking for help in a very passive way, showing their somatic complaints and symptoms and making many specialists impotent. And if they are referred to a psychotherapist they will say: "My illness is in my belly or in my back, but not in my head". Such a patient could even feel devalued or hurt by the advice to see a psychotherapist.
Case study
A 48-year-old man is coming to see me, a father with three nearly grown-up children, in a good professional position, who complains about lowerback pain, which has bothered him for ten years. In the X-rays there are only a few degenerative signs In the vertebrae of his lower back, many therapies in and out of hospital did not help him, he had also tried practically all pain-killer drugs and antirheumatic substances. Because of his chronic pain he had stopped physical sporting activities and he was very often away from work, not only because he had to see his physicians or therapists, but also because of his symptoms, which would force him to stay in bed. While I was talking to him, he showed no problems in life, by the way he said that his wife was ill and suffering a rheumatoid disease and that she had heart problems, his children were developing very well and presented no problems. Also at work everything seemed to be okay: he is working in a responsible and leading position and he is under stress very often, but he felt that this is a normal thing in these times. As with all patients, I examined him physically as well. I realized that Irom the medical point of view he was in perfectly good health, except for his lower-back pain. On contact I realized that he looked very unhappy: his eyes looked worried and without brightness, his look hung on me as if he was asking for something, his voice was monotonous and low, his face was looking at me but practically without feelings expressed while he was talking. His body looked tall, slim and, from the side, he showed a typical sign of kyphosis and lordosis which indicated some collapse Ln his longitudinal axis. His legs, especially in the lower half, were slim and like sticks, his feet were collapsed in the arch. His sternum was slightly collapsed, his breathing was superficial and the breathing movements were practically invisible. When I touched the muscles on his arms or legs there was considerable tension, also in his shoulders and neck. His hands and feet were cold and, while he was standing, his legs showed a bluish colour without signs of varicosis.
Although I suspected a psychosomatic illness, neither in his childhood biography nor in the family history could evidence be found that could have supported such a hypothesis. I knew only that all the earlier treatments lik physiotherapy, medication and acupuncture had not helped. If I had referred the patient to a psychotherapist, he probably would have said : "My illness is in my back and not in my head, I am not crazy !". Perhaps he would have got very angry at me and he would have left my office protesting and perhaps he would have gone to see his 17th physician. I said to him that I would like to try a few exercises, in order to understand his illness better. He accepted and so he came for his second appointment.
Firstly, I asked him to try an exercise with me in order to get more into contact with his legs. I asked him to bend his knees while exhaling and to stretch his knees while breathing in. With this exercise he started to breathe deeper. Then I asked him to bend over forward while touching the floor with his hands, and to stretch his knees while exhaling. This exercise stretched his lower-back and the posterior muscles of his legs. After a few exercises, which stretched chronic tensions in his lower—back, a sudden emotional break-through happened, the patient let himself fall to the floor and started to cry deeply.
Then he told me how much he was suffering with the illness of his wife, he felt overwhelmed by the tasks of his life, and at the same time left alone. All of a sudden his whole unhappiness was visible not only to me but also to him. Without difficulty he suddenly remembered how he had been left alone by his mother as a child, because she had to work, and how he had to learn early to stand on his own feet. For a moment his chronic pain in his back had disappeared and, talking, he realized how the emotion, in this case the sadness, had caused the chronic tension in his back and his pain.
This was the beginning of a therapy where the patient learned exercises to practise at home, which were taught to him to work with the chronic tension in his legs and in his lower back, and to give him a feeling for more grounding. In terms of a focal therapy his symptoms disappeared completely within a year. The patient started to do sports again, to swim and cycle. Therapy stopped five years ago; I saw him recently and he had had a small relapse, which could be helped by a few more sessions.
This example shows how bioenergetic analysis ran be integrated into psychosomatic medicine. Like always, a clear diagnosis and a therapy plan precede the therapeutic work. In this example the deprivation in early childhood could be read already on the body in terms of character-structure signs of an oral personality. Typical for this condition is the picture of the child standing on his own feet too early, although the muscles are insufficiently developed. The infant is asked to be independent and to support himself, because mother cannot give enough attention.
Besides the collapsed feet and the sticklike legs, we find a collapsed chest and chronic tension In the shoulders. Such children learn very early not to stretch their arms towards the mother because they have to learn early that this movement does not help much with a mother who has little emotional presence. In our example it is also typical that the pain in the back starts at the moment when the wife of our patient gets sick from polyarthritis and,
with this sickness, an emotional support in his life is taken away: when his balance in his life was still enough, the illness of his wife caused chronic overweight in his lower-back, which caused his pain. This example shows also clearly two things: working psychosomatically means to work with primarily "unmotivated patients" and it is possible to work in a short-term therapy if certain preconditions are fulfilled.
4. COMMON PSYCHOSOMATIC SYNDROMES
As already mentioned above, 50 to 70 percent of all patients in general practice or in internal medicine are suffering from psychosomatic disease. They are a big problem in the public-health system, because they create constantly new costs, diagnostically and therapeutically, and nobody can really help them. The famous colitis ulcerosa, anorexia nervosa, asthma or gastric ulcer are relatively rarely seen. They are the classical diseases everybody thinks of when we speak about
psychosomatic illnesses. But much more common are complaints like: repetitive infections of the throat, the sinuses, the bronchial system, or the bladder, cardiac pain or disturbances of heart rhythm, high blood pressure, functional pain of the belly like irritable colon, or hyper-secretory gastritis, rheumatoid diseases, pain of joints or muscles and tendons, lower-back pain, sexual disturbances, headaches. Working with patients with such complaints in the last eleven years I have been very aware of how I) bioenergetic analysis helped me to understand quickly and work focused with these patients. Paragraphs 5 - 9 will illustrate how bioenergetics can be integrated into psychosomatic medicine.
5. REPETITIVE INFECTIONS
Here it is clear that two pre-existing conditions can influence the development of an inflection. A block in the affected area or depression of the immune system. So therapy has to Influence both sides. With repetitive infections of the throat, we will work on the neck and throat to the 1 p the person to release the tension, which Impairs the blood flow and therefore makes the throat a place of minor resistance in the view of the bacteria or viruses; for the therapist the same place is characterized by major resistance. The same concept is adapted to chronic sinusitis: work with this part of the body means working with the blocked sadness, the secretion of the mucous within the sinuses is connected to the tear gland and, if the secretion of the mucous in the sinus is reduced or the liquid is too thick, the constant cleaning mechanism of the sinuses is impaired. Letting the patient get rid of his blocked sadness will stimulate the production of the mucous. In a similar way we can look at chronic urinary infections, but there we will have to look carefully at the way sexuality is integrated or suppressed in the life of (his patient. To reinforce the capacity of the immune system we will have to stimulate the right brain. There In some evidence that it is from this side that the hypothalamus is suppressed or activated, a most important center in coordinating the actions of the very complicated immune system (2). But now can we stimulate the right hemisphere of the brain? Either through relaxation and meditative exercises or through diminishing the dominance of the left brain, the responsible part of the logic system, the analytical, verbal descriptive part of the personality. The right brain represents the nonverbal expression and comprehension, it is more holistic, synthetic, room-visual oriented, intuitive, without feeling of time, and unfocused. Somehow, we will have to influence the balance between left and right brain in terms of increasing the energy of the right brain (3).
In clinical research concerning the therapy of patients with malignant tumors, much evidence has been put together that psychotherapy prolongs the life of cancer patients significantly. Whether this happens through stimulation of the immune system by psychotherapy needs still more research and proof. What has been proven recently by Barbara PEAVEY (4) is that relaxation techniques, even in the short term, can improve the quality of immune response measured with blood samples (phagocytic functioning of white blood cells).
6. SYMPTOMS OF THE CARDIOVASCULAR SYSTEM
In these people we find in terms of bioenergetics very typically blocks in the chest which are seen through restriction of respiration but also can be palpated as muscle tensions in the rib muscles. There is decreased mobility of the chest and very often much tension around the shoulders. In terms of character structure, we find here psychopathic character traits over-represented. In contact these patients have difficulty in showing love and i respect for their partners. Reaching out and asking lor help is nearly impossible and very often connected with much anger. Love comes from the heart and opening the heart means letting love and tender feelings flow into everyday life. In short-term therapy, therefore, working with couples and I nr I tiding the partner of the patient means bringing the conflict into the therapy room and working directly with the blocked feelings. If anxiety is connected to a fast heart rate, working with reinforcing the support of the patient would make »'out sense. There we would work with grounding exercises to re-establish the sense of standing on one's own feet.
In hypertension, also a disease of the cardiovascular system, there are many theories about the psychodynamic conflict behind this condition. As 20 percent of the grown-up population in civilized countries suffer from hypertension, we call this, not an illness, but a condition created by a certain lifestyle. The hypertensive patient has difficulty in dealing with stressors, he cannot keep his boundaries and he is unable to defend himself u a Inst the challenge of his surroundings. Anger is very often held in and provides the patient with more of a sense of inner stability. Physiologically speaking, the arteries of such a patient are stiffer because the blood pressure is higher. Relaxation of the whole organism through awareness, energetic exercises, and relaxation technique, should reach i in deepest levels of the tissue in the body, and only then will the blood pressure slowly decrease and reduce the high risk of chronic hypertension. In the transference process themes of dependence and independence were shown to be a crucial issue in the III«- of these patients.
7. FUNCTIONAL DISTURBANCES OF THE DIGESTIVE SYSTEM
Colon irritabile (painful tensions in the muscles of the large intestine), diarrhoea or constipation, hypersecretory stomach, disease of gall bladder but also gastric and duodenal ulcer, hiatus hernia, are the most common symptoms of the gastrointestinal tract. We find these patients very difficult because they often suffer from masochistic traits and oral disturbances as well. A block in the diaphragm, which stops the flow of energy in the longitudinal axis, is often visible in body reading, often combined with paradoxic breathing, where belly and thorax work in a contrapulsatory way. To correct paradoxic breathing helps the pain quite quickly. Twenty times per minute the diaphragm, if unblocked, pushes the intestines down and the wall of the belly out so that the intestines are compressed and expand in a rhythmical way. This massage mechanism is important for the relaxation of the intestinal muscles which are under control of the solar plexus and the vegetative nervous system.
But also in the pelvic girdle we will find blocks and in the whole pelvic area. Working with the repressed sexuality will open up the blocks and free the chronic tension in the peritoneal muscles and the muscles of the pelvic area.
8. RHEUMATOID DISEASES
Here muscles and the skeletal system are involved. The inflammatory rheumatoid symptoms, like chronic polyarthritis, make up only 7 percent of the whole rheumatoid syndromes. Fifty-five percent is the so-called extra articular rheumatism (pain in muscles and tendons), 38 percent are arthrosis and therefore degenerative forms of rheumatism. The inflammatory rheumatism, the true polyarthritis, is connected to what I mentioned above about the immune system. It is an auto-aggressive immune-system disease, and therefore needs working with reinforcing the balance of the immune system.
In tendons and muscles, the organs of movement, impairment of motility is in the foreground. We may find stiffness or even calcifications or flaccidity. These symptoms are best seen as rigid blocks in the personality, which have the function to provide a sense of coherence to the individual. KELEMAN (5) in his new book "Emotional Anatomy" describes clearly the two different fibres in muscles, the quick and pale fibers and the slow and red fibers with extra haemoglobin. The latter can only be influenced to release their tension by what he calls "parenting". Giving a sense of deep trust and nurturing is afforded, which often will lead the patient into a long-term psychotherapy, either single or in groups. The fast fibers are for rapid action such as immediate response or the quick patterns of the startle reflex that provoke attention. The slow fibers are necessary for postural and social stance that provide a sense of stability and reliability. Deep or slow muscle patterns represent our stable self. Emotional relearning is not to be confused with muscle relaxation for the fast-acting group.
The affected joint represents the schizoid part of the problem. The joints are places where people are connected, one part to the other of the body. Joints have a lubricant, a liquid, which helps to smooth the movement and both protects and nourishes the cartilage of the joint. In arthrosis it has been shown that the qualities of the lubricant are disturbed. The liquid is waterier and has less proteins and condroitin sulphate acid, so that the cartilage is undernourished and degenerates too quickly. We know that the cells of the inner layer of the joint capsule produce this liquid with the right viscosity, if the blood supply to these cells is not reduced. So tensions in the small muscles around the joints will cut and reduce blood flow in the capsule and therefore the cartilage is undernourished and abused and will be destroyed too early. In addition, the increased tension in the movement muscles will create too much pressure in the contacting parts within the joint. This will make outside pressure to the organism unsupportable to the cartilage cells and therefore create microtraumas in the joint cartilage, creating a new source of early degeneration.
Therapy will have to influence these structures by working with schizoid blocks, with repressed terror and anger and, of course, with a lot of well dosed support and nurturing. Especially if grounding is insufficient, the patient needs to work on his feet and legs. All different kinds of grounding have to be brought into awareness.
9. RESPIRATORY SYSTEM
Free and full breathing provides oxygen to the organism, this is the most important energy supply. But breathing is also a movement, and thin represents the mechanical part of the process. Open breathing provides an open sense of reality, which is important to keep in mind while working with depressive patients (6).
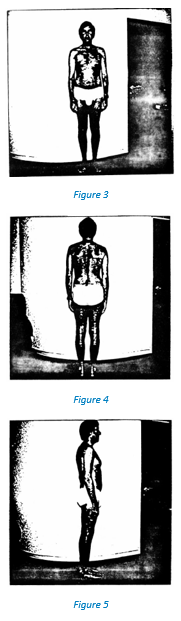
The captured breathing can also be shown very easily by measuring the dynamic pulmonary function (fig. 2). This figure shows the values of a man born in 1942, before starting therapy (column under 04.06.1982), after a bioenergetic session dealing with his breathing (column under 15.06.1982) and one year after ending therapy (column under 12.02.1986). FVK measures the functional vital capacity, that means the volume of air taken in with a full maximum breath in millilitres; FEW 1 is the forced expiratory volume in the first second of expiration, PF the peak flow of air in litters per minute. AGV means the maximal ventilation volume per minute with quick and deep breathing. What strikes immediately in the first column (04.06.1982) is a very low FEV 1 of minus 951 millilitres, which is usually only seen with asthmatic conditions. The reduced FVK of minus 173 represents the reduced volume because of much tension and stiffness in the chest.
In fact, the body of this patient attracts our attention in two important places (fig. 3 - 5). A constriction in the chest and diaphragm with slight collapse of the sternum, and slim and stiff parts around the ankles. Many other important signs can only be seen in the original photograph. The man was referred to me for psychosomatic diagnosis and therapy by a colleague who had tried to treat him for two years with different kinds of drugs because of multiple vegetative symptoms creating disturbances of the heart rhythm, fear of heart infarction, hyperventilation attacks, and subjective feeling of not having enough air to breathe. In the body we can see the restricted respiration and the sense of not being grounded enough, and therefore the fear of falling. In the therapy-session of 15.06.82, while working with the breathing on the stool, the patient remembered suddenly that as a
|
K.U.. 1942 |
Normal Value |
4.6.1982 |
15.6.1982 |
12.2.1986 |
|
FVK/CVF (ML) |
4993 |
- 173 |
+ 1527 |
+527 |
|
FEVl/VEMS (ML) |
4231 |
- 951 |
- 281 |
+1209 |
|
PF/DEH (L/MIN.) |
566 |
- 135 |
- 147 |
- 90 |
|
AGW/VMM |
182 |
- 18 |
- 18 |
- 15 |
Figure 2
child he had suffered from asthma, which disappeared in his first years at school. After this session much tension in his thorax was gone and therefore, we find an FVK of 1527 millilitres. The FEV 1 of minus 281 vs. minus 951 represents a marked decrease in the chronic tension of his bronchial muscles which are connected to the vegetative nervous system. After ending therapy this value even increases to plus 1209, which means that more of his internal tension located around the bronchial system has been released than in the thoracic muscles. Also FVK and PF have markedly increased through therapy; as to AGV, we did not expect much change, the value of minus 18 litres per minute not being significantly decreased. PF and AGV still being slightly under the normal value has no clinical relevance.
After therapy we find also the body shape changed, the legs are fuller around the ankles, the diaphragm is not constricted so much anymore, the breathing pattern is smoother and includes belly and thorax at the same time of the breathing cycle. The vegetative symptoms which were impairing the working capacities of the patient had disappeared and also his depressive mood gave way to more pleasure in life and in his relationships.
10. SHORT-TERM BIOENERGETIC PSYCHOTHERAPY
As already mentioned, short-term psychotherapy is important in psychosomatic medicine. It is the expression of the will of the physician to treat efficiently and cheaply. Short-term psychotherapy (STP) last for 3 to 30 sessions per patient; it is limited in time right from the beginning. The psychoanalytical literature defines criteria for the indication of STP. Basically, we can summarize them in three main criteria (7, 8):
- the patient has to be motivated for therapy; he has already enough insight to know that his symptoms are psychological;
- the patient has to be well integrated in his life and to have enough personal support; the symptom must not be chronic and therefore have lasted for too long;
- there must be a clear focus or conflict which must explain the source of the disease psychodynamically. In addition, the conflict must be near enough to the awareness of the patient.
These criteria have been proven to guarantee some success in therapy within the framework of psychoanalysis. I apply the same criteria to bioenergetic short-term psychotherapy, but with bioenergetic analysis these criteria are dealt with differently In exploring the indication of short-term psychotherapy.
a) Motivation
We work directly with the afflicted part of the body, with the lower back of the patient, with his belly, or with his tensions in the breathing system. The psychosomatic patient feels that he is taken seriously by the therapist when the symptom itself can be part of the work physically and psychoIogically.
b) Integration and support
Body reading gives us an easy way of diagnosing these two criteria. We look at the legs, which represent directly the support available to the person. How and whether the person is giving himself enough support is crucial to the outcome of therapy. An ungrounded person needs much nurturing and is apt to develop a new symptom if we work with STP, even if the therapy seems to be a success because the first symptom which brought the patient to therapy disappeared. Very quickly we get the sense of the integration of the person in the world by body reading.
c) Conflict or block
Also in this respect we get a clear image of the main block with which we have to work. We will work with the main symptom and get quickly a clear sense of the hidden conflict. The emotion will be discharged and the content of the conflict then expressed and worked through verbally. Too many superimposed blocks are usually a contra-indication for STP and need long-term psychotherapy.
This following last example illustrates how to deal practically with these criteria. 33-year-old medical professional women comes to see me because of endometriosis with strong pain in the lower abdomen. Her gynaecologist had proposed an operation, the diagnosed infertility in 10 years of living together with a man had been explained by the endometriosis. Before taking the decision to have the operation done because of the pain, the patient, knowing about the psychosomatic connections, wanted to try body work (she had attended one of my workshops a year before she came to see me). In body reading I found her well-integrated in the world, with enough support in her own legs, the body being not too imbalanced, some schizoid traits in her eyes were visible. Striking were the underdeveloped female parts of the person represented by tension and immobility in the pelvis. The therapy was focused on confrontation with a castrating mother and the looking for acknowledgement by the father. After 10 sessions, to her and my surprise, she was pregnant after she had been living with her man for 10 years. During pregnancy more work with being accepted through the mother in herself was done; the birth of the child went very well and the therapy stopped in an natural way.
In summary my purpose is to show that concepts of somatic medicine can be connected to concepts of bioenergetic analysis. The translation of terms and concepts in bioenergetic analysis to somatically orientated medicine is possible. Energy, a term which I very often used in bioenergetic analysis, can be translated into flow of blood, oxygen supply, movement of muscles, tendons and joints, metabolic streams in nerves, and can also be measured with certain functional tests. This more somatic understanding of bioenergetic analysis can help people Irom the medical profession to understand more quickly in their language what bioenergetic analysis means. Therefore, bioenergetic analysis is an Important enrichment for diagnosis and therapy in psychosomatic medicine.
References
- Von UEXKULL Thure: Lehrbuch der Psychosomatischen Medizin. Urban + Schwarzenberg, München - Baltimore, 1979.
- ADER Robert: Psychoneuroimmunologie. Académie Press Inc., Orlando, Florida, 1981.
- HAMPDEN-TURNER Charles: Maps of Mind. Beazly Publishers Ltd., London, 1981.
- PEAVEY Barbara: Journal for Biofeedback and Self-Regulation. 10, 33-47, 1986.
- KELEMAN Stanley: Emotional Anatomy. Center Press, Berkeley, Ca. 94709, 1985.
- LOWEN Alexander: Depression and the Body. Coward, Me Cann & Geoghegan Inc., New York, 1972.
- BECK Dieter: Die Kurzpsychotherapie. Hans Huber, Bern, Stuttgart, Wien, 1974.
- SIFNEOS Peter E.: Short-Term Psychotherapy and Emotional Crisis. Harvard University Press, Cambridge, Mass., 1972.

